Why CPAP Mask Fitting Needs More Than S, M, and L
How AI-assisted scan analysis, mask-specific size rules, patient questionnaire inputs, and structured top match lists can help reduce avoidable refits and simplify CPAP mask selection.



Key takeaway
CPAP mask selection is not a simple Small, Medium, or Large lookup. MaskFit AR uses AI-assisted scan analysis, patient questionnaire inputs, and mask-specific sizing intelligence to create a structured top match list and help teams reduce avoidable fit-related refits to less than 5% without replacing clinician judgment.
Digital mask fitting starts with better mask intelligence
Digital CPAP mask fitting depends on several inputs working together: a useful patient scan, reliable mask sizing intelligence, and relevant patient-reported fit factors. A scan can provide patient-specific fit data, but that data only becomes actionable when it is interpreted against the right mask-specific sizing rules. AI-assisted scan analysis can help make this interpretation more consistent by supporting the extraction and review of fitting-related data from the scan. This matters because CPAP masks are not sized consistently across manufacturers or interface types. A Medium in one product family may not map to a Medium in another. Some masks use traditional Small, Medium, and Large sizes, while others include Petite, Extra Small, Wide, Medium Wide, Small Wide, Standard, Regular, One Size, or combined sizes. For this reason, the fitting workflow should not depend only on a printed size label. It should help interpret the patient’s facial measurements against the sizing logic for each mask and size.Why mask selection is more complex than it looks
Across a multi-manufacturer CPAP mask catalog, size labels and fit rules can vary by product family, interface type, cushion geometry, and design intent. AI is useful in this workflow because multiple inputs must be interpreted together rather than reviewed as isolated size charts. This creates several practical challenges for providers:- Size labels are not universal: the same label may represent different physical fit ranges across different masks.
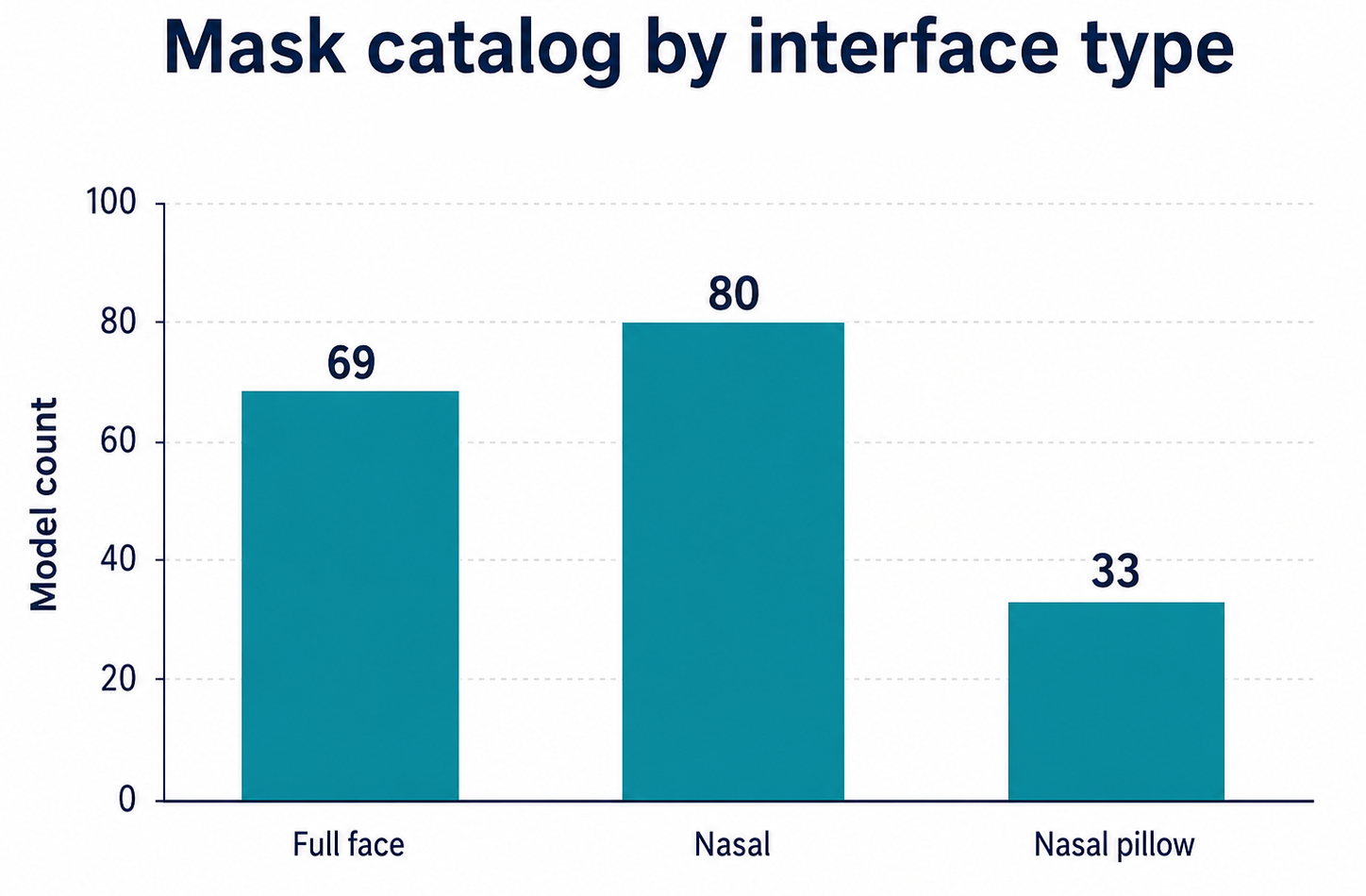
- Interface types use different logic: full face, nasal, nasal pillow, and minimal-contact masks may rely on different parts of the face.
- Boundary cases are common: a patient may fall near the edge of one size and close to the start of another.
- Width variants matter: some patients may need Wide, Medium Wide, Small Wide, Petite, or other alternate cushion styles.
- Manual review can be inconsistent: staff may need to compare multiple charts, brands, and mask families before making a selection.
The refit challenge
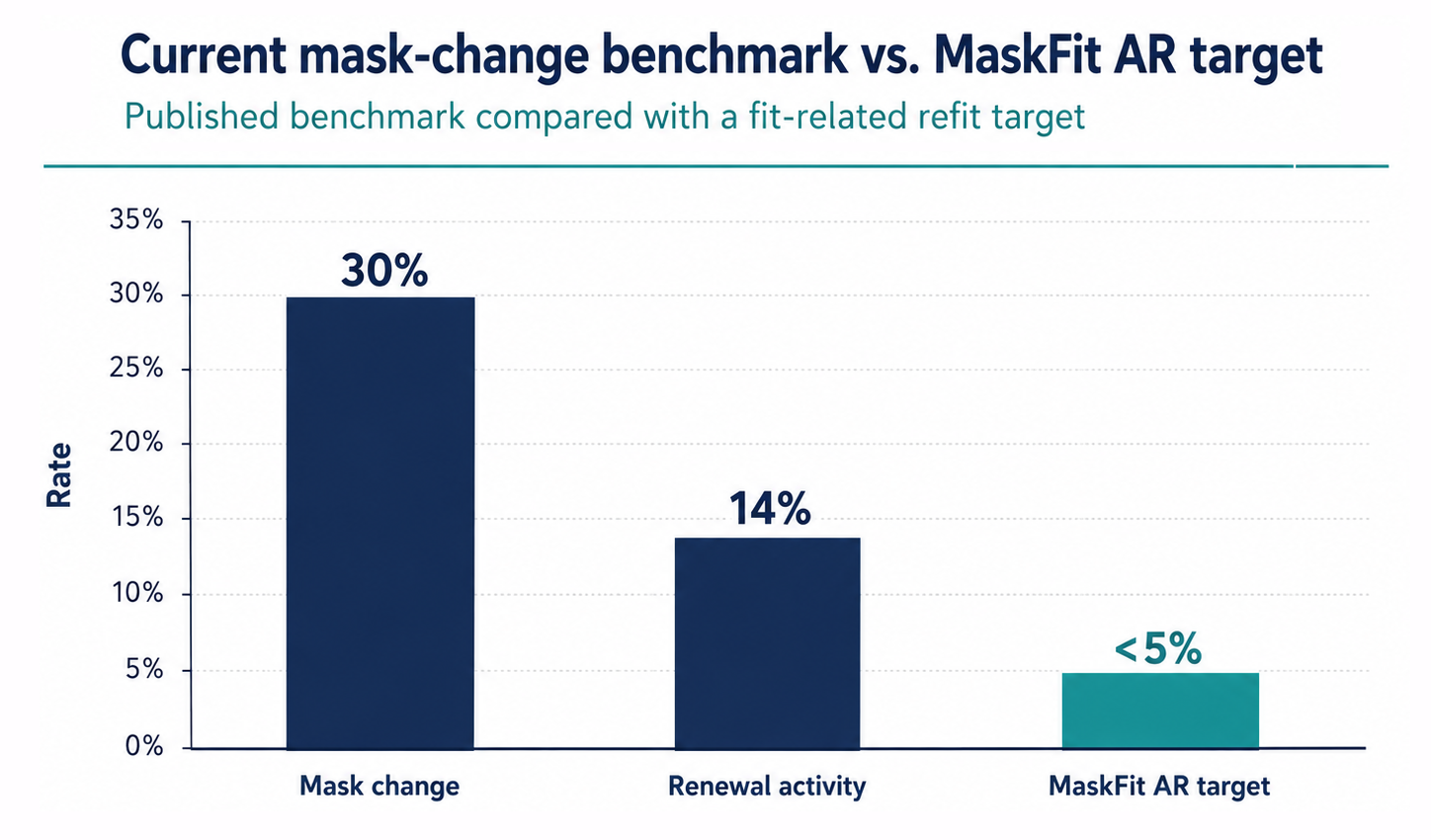
Mask changes and replacements are common during PAP therapy. Published PAP data has reported that 30% of patients changed masks within less than one year of starting CPAP, while another 14% had mask renewal activity that may have involved a different size or brand within the same mask type [1] [2]. Additional research has also shown that, among patients using PAP for less than four hours per night on their first mask, mask change or renewal was associated with increased device use after the intervention. The same study identified the first 90 days as an important window for addressing mask-related issues in patients struggling with therapy use [3]. These public findings are not the same as MaskFit AR’s fit-related refit rate. Mask change, mask renewal, routine replacement, and fit-related refit are different measures. However, they show that mask selection often continues to evolve after therapy begins. MaskFit AR focuses specifically on avoidable fit-related refits: cases where a patient requires a different mask or size because the initial mask match did not work as expected. Based on internal MaskFit AR outcome data, fit-related refits can be reduced to less than 5% when MaskFit AR is used as part of the fitting workflow [4].How fit-related refit rate is measured
Fit-related refit rate = patients requiring a different mask or size within 30 days of the initial mask match divided by total patients fitted through the workflow.
How MaskFit AR helps reduce avoidable refits
MaskFit AR is designed to reduce avoidable fit-related refits by improving the initial mask match. Instead of asking staff to manually interpret every sizing guide, the platform uses AI-assisted scan analysis, mask-specific sizing intelligence, and patient questionnaire inputs to narrow the catalog and present a structured top match list for review. This matters because mask fit is not based on facial measurements alone. Factors such as nasal congestion, seasonal allergies, deviated septum, preferred sleep position, facial hair, skin sensitivities, claustrophobia, and magnet-related restrictions can all influence which mask style may be most appropriate for a patient. The goal is not to guarantee that every first mask will be perfect. Comfort, seal, therapy pressure, product availability, clinical context, and patient preference still matter. AI is used as decision support, not as a replacement for clinical judgment. The goal is to reduce preventable mismatch by combining scan data with relevant patient-reported factors, making the initial mask selection more data-driven, consistent, and easier to review. With a structured scan-to-match workflow, MaskFit AR helps organizations reduce avoidable fit-related refits to less than 5%, based on internal outcome data and a clearly defined refit measurement window [4].How MaskFit AR narrows the mask selection
At a high level, the MaskFit AR workflow helps move teams from broad catalog review to ranked, clinically reviewable mask options:- Patient scan: the patient completes a guided scan in-office or remotely through a secure workflow.
- Questionnaire inputs: the patient provides relevant fit information, such as nasal congestion, allergies, deviated septum, sleep position, facial hair, skin sensitivities, claustrophobia, and magnet-related restrictions.
- AI-assisted fit analysis: the platform interprets scan-derived data and patient-reported factors together before the catalog is narrowed.
- Fit data extraction: the scan produces fitting-related measurements used for mask comparison.
- Mask sizing comparison: the system compares the patient’s fit profile against mask-specific size rules.
- Top match list: compatible masks and sizes are filtered and prioritized for clinician review.
- Clinician confirmation: the final selection can account for clinical context, product availability, patient comfort, and patient preference.
Why ranking matters
A simple pass/fail result is not enough for CPAP mask fitting. Two mask sizes may both appear compatible, but one may align more closely with the patient’s measured fit profile while another may sit near the edge of its sizing range. AI-assisted ranking can help make those differences easier to review by organizing compatible options into a clearer top match list. Ranking also supports backup options. If the first mask is unavailable, not preferred by the patient, or not ideal after clinician review, the team can consider the next strongest option without starting the selection process over manually.Manual fitting vs. MaskFit-assisted fitting
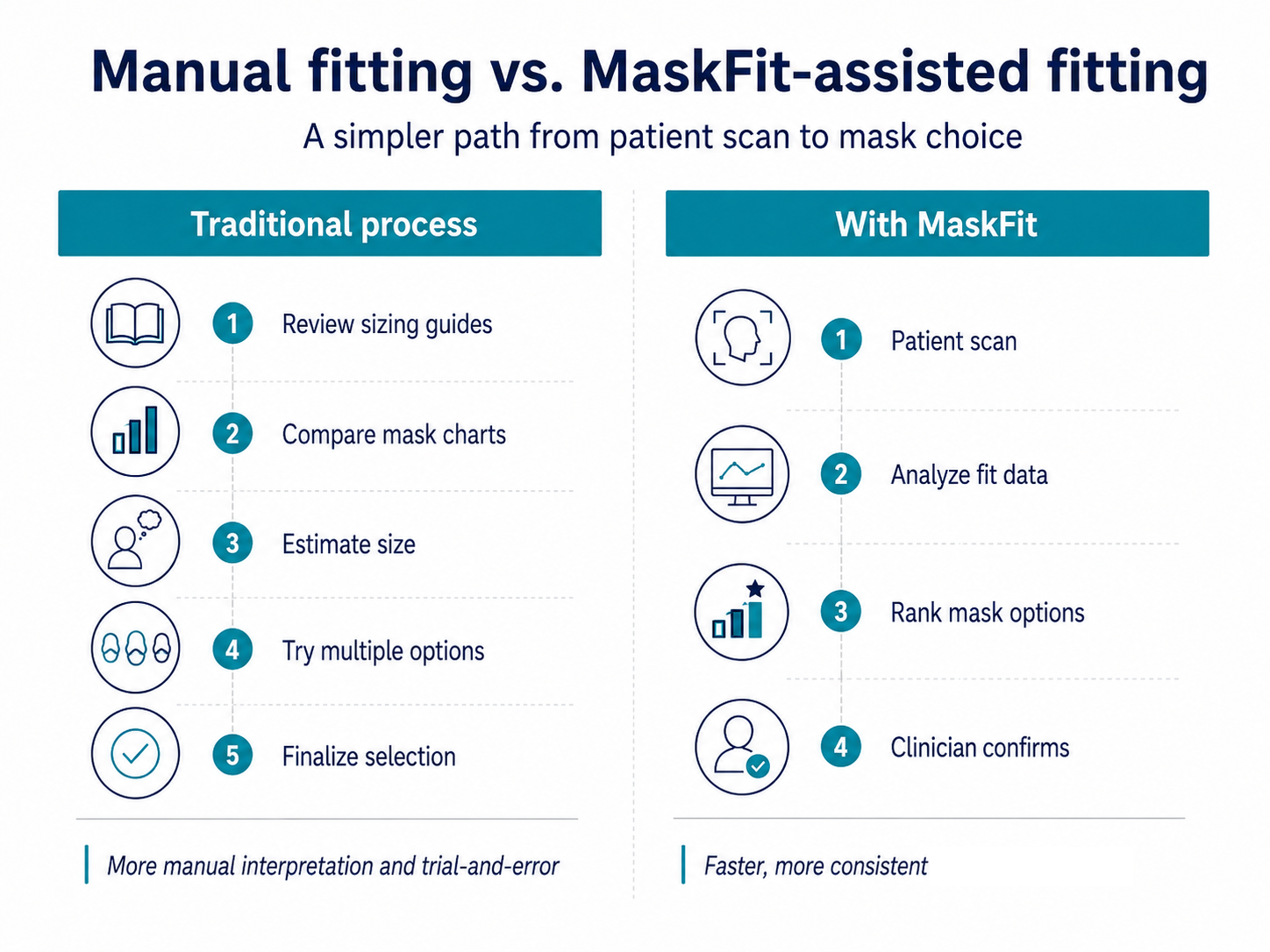
Traditional mask selection often requires staff to review sizing guides, compare charts, estimate a size, try one or more options, and then adjust if the first choice does not work. That approach can be effective, but it depends heavily on manual interpretation and staff experience. MaskFit AR helps move the analysis earlier in the workflow. AI-assisted scan analysis and mask-specific sizing logic can filter the catalog first, allowing the clinician to review a more focused set of options instead of starting from the full mask catalog.How the top match list should be used
MaskFit AR supports the fitting process by creating a structured top match list based on scan-derived fit data, patient questionnaire inputs, AI-assisted fit analysis, and mask-specific sizing logic. The final mask choice may still depend on patient preference, clinical input, product availability, pressure requirements, and follow-up experience. This distinction matters. The purpose of the top match list is to support a more informed and consistent selection process, not to replace professional judgment or the patient’s comfort feedback.The path forward
As digital CPAP mask fitting continues to evolve, the value of the workflow will depend on how well patient scan data, questionnaire inputs, mask-specific sizing intelligence, and AI-assisted fit analysis can be combined. A large catalog is useful only if teams can quickly narrow it to the most relevant mask and size options for each patient. For MaskFit AR, this is a central product direction: turning complex mask sizing intelligence into a clear, scan-based matching workflow that helps patients, clinics, DMEs, manufacturers, and online sellers make more consistent mask-selection decisions. By improving the initial mask match, tracking fit-related refits over time, and using AI to identify patterns in fit outcomes, organizations can create a more scalable fitting workflow and reduce avoidable refits to less than 5%.References and source notes
This article is for general education and workflow discussion only. MaskFit AR supports the mask fitting process, but final mask selection should account for clinician judgment, product availability, patient comfort, therapy requirements, and follow-up experience.- Genta PR, Rosanelli I, Morgenthaler TI. Time to Change: The Effect of Mask Switching on Continuous Positive Airway Pressure Adherence. Annals of the American Thoracic Society. 2025;22(1):41–42. View reference
- Schoebel C, Woehrle H, Ficker JH, Graml A, Zeman F, Fietze I, Young P, Arzt M. Effects of Mask Change/Renewal on Adherence to Positive Airway Pressure Therapy: Analysis of a Large Telemedicine Database. Annals of the American Thoracic Society. 2025;22(1):130–137. View reference
- Simonsen S, Staley B, Bae C, Schutte-Rodin S. The Effect of Changing the First CPAP Mask on Compliance. Sleep. 2018;41(suppl_1):A399–A400. View reference
- Internal MaskFit AR outcome data. Fit-related refit rate measured as patients requiring a different mask or size within 30 days of the initial mask match, excluding routine resupply, non-fit-related replacements, and inventory substitutions. Analysis period: 2025. Sample size: approximately 40,000 patients.